Clinical Science | Trauma
A Ali, O Olubowale, D Tatum, P McGrew, J Duchesne, S Taghavi
ePoster Presenter: Ayman Ali Ali BS, Tulane School of Medicine
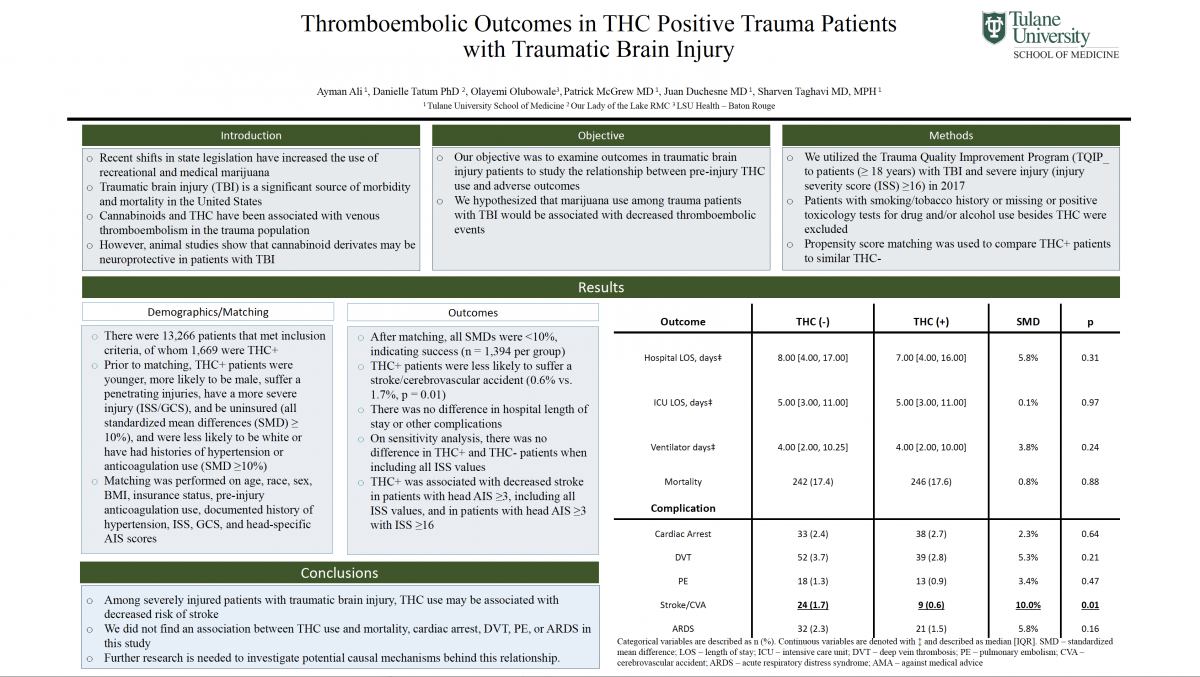
Background: Traumatic brain injury (TBI) is a significant source of morbidity and mortality in the United States. Recent shifts in state legislation have increased use of recreational and medical marijuana. While cannabinoids and tetrahydrocannabinol (THC) have anti-inflammatory effects, whether pre-injury use of THC impacts severe TBI is unknown. We hypothesized pre-injury THC use in trauma patients suffering TBI would not improve patient outcomes.
Objectives: To determine if THC use was associated with clinical outcomes in patients with TBI.
Methods: The American College of Surgeons Trauma Quality Improvement Program (TQIP) was used to identify patients aged ≥18 years with severe TBI (Glasgow coma scale (GCS) ≤ 8) in 2017. Patients with missing drug screen information or positive for drug and/or alcohol use besides THC were excluded. Demographic variables and injury patterns were examined using Chi Square analysis for categorical variables and the Wilcoxon-Kruskal-Wallis test for continuous variables. Multivariate logistic regression was used to determine if THC use was associated with clinical outcomes.
Results: A total of 4,426 patients that met inclusion criteria, of which 774 (17%) were positive for THC only. Compared to patients with no drug or alcohol use, THC+ patients were younger (median age 27 years vs. 54, p < 0.001) and more likely to be male (86% vs. 70%, p < 0.001), uninsured (20% vs. 12%, p < 0.001), nonwhite (38% vs. 26%, p < 0.001), and victims of assault (15% vs. 5%, p < 0.001) or firearm injury (19% vs. 7%, p < 0.001). There was no difference in initial GCS (median 3, p = 0.214) between the groups, although THC+ patients had significantly longer intensive care lengths of stay (median 6 days vs. 5, p = 0.01), days on a ventilator (median 5 days vs. 4, p = 0.04), and hospital days (median 9 days vs. 7, p = 0.01). THC+ patients had significantly lower mortality rates (42.9% vs. 51.5%, p < 0.001) and, although not statistically significant, fewer pulmonary embolisms (PE) (0.5% vs. 1.3%, p = 0.08), fewer strokes (1.2% vs. 2.4%, p = 0.05), and higher rates of ventilator-associated pneumonia (7.5% vs. 5.7%, p = 0.06). On multivariate analysis controlled for age, injury severity, method of payment, gender, race, and THC use, being THC+ was not associated with mortality (odds ratio (OR): 0.95; 95% CI: 0.78 – 1.14, p=0.56), but was associated with decreased odds of PE (OR 0.29; 95% CI: 0.09 – 0.76, p = 0.02) and stroke/cerebrovascular accident (OR 0.44; 95% CI: 0.20 – 0.86, p = 0.03).
Conclusion: Pre-injury THC use may be associated with decreased clot burden that leads to less PE and cerebrovascular accidents in patients with TBI. Further research in pathophysiological mechanisms related to THC use and TBI are needed.