Clinical Science | Surgical Oncology
B Campbell, M Aboueisha, A Attia, M Omar, N Mankowski, E Toraih, M Shama, E Kandil
ePoster Presenter: Brett Campbell BA, Tulane School of Medicine
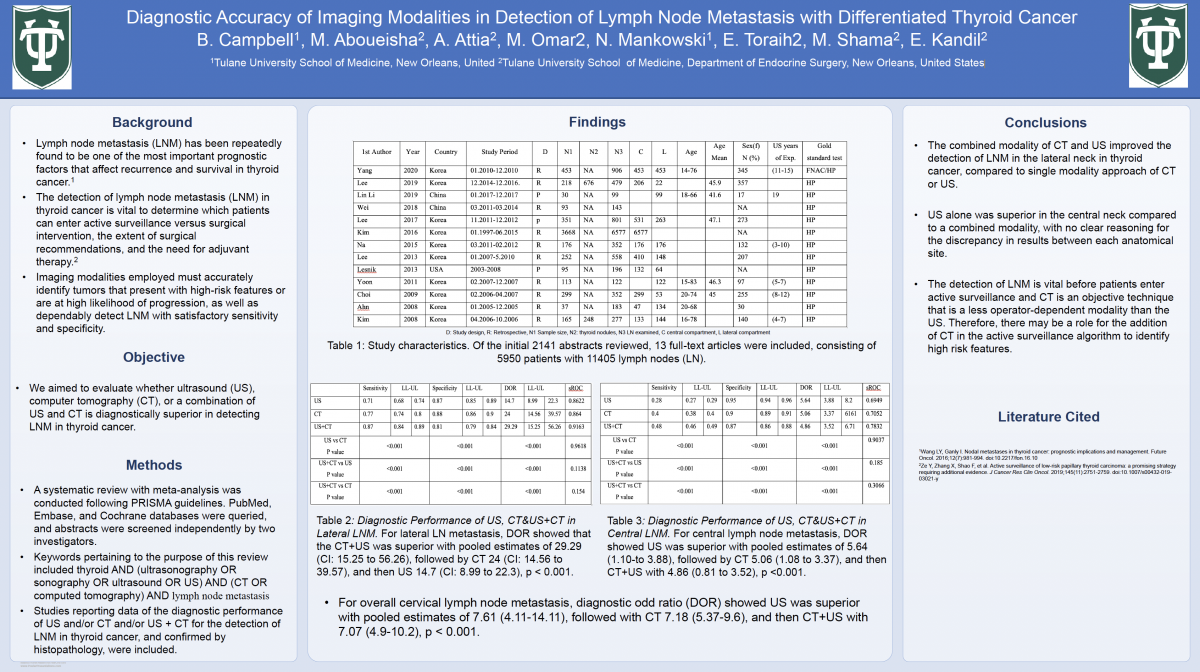
Background: The detection of lymph node metastasis (LNM) in thyroid cancer is vital to determine which patients can enter active surveillance and which require surgical intervention.
Objectives: We performed a meta-analysis to evaluate whether ultrasound (US), computer tomography (CT), or a combination of US and CT is diagnostically superior in detecting LNM in thyroid cancer.
Methods: Following PRISMA guidelines, PubMed, Embase, and Cochrane databases were queried, and abstracts were screened independently by two investigators. Studies reporting the diagnostic performance of US and/or CT and/or US + CT for the detection of LNM in thyroid cancer, and confirmed by histopathology, were included.
Results: Of the initial 2141 abstracts reviewed, 13 full-text articles were included, consisting of 5950 patients with 11405 lymph nodes (LN). Analysis of the diagnostic performance of CT, US, and CT+US in overall cervical lymph-node metastasis, lateral lymph node metastasis, and central lymph node metastasis was performed. For overall cervical lymph node metastasis, diagnostic odd ratio (DOR) showed US was superior with pooled estimates of 7.61 (4.11-14.11), followed with CT 7.18 (5.37-9.6), and then CT+US with 7.07 (4.9-10.2), p < 0.001. For lateral LN metastasis, DOR showed that the CT+US was superior with pooled estimates of 29.29 (CI: 15.25 to 56.26), followed by CT 24 (CI: 14.56 to 39.57), and then US 14.7 (CI: 8.99 to 22.3), p < 0.001. For central lymph node metastasis, DOR showed US was superior with pooled estimates of 5.64 (1.10-to 3.88), followed by CT 5.06 (1.08 to 3.37), and then CT+US with 4.86 (0.81 to 3.52), p <0.001.
Conclusion: The combined modality of CT and US improved the detection of LNM in the lateral neck in thyroid cancer, suggesting there may be a role for the addition of CT in active surveillance to identify high risk features.