Clinical Science | Patient Safety
C Becnel
ePoster Presenter: Chad Becnel MD, Tulane School of Medicine
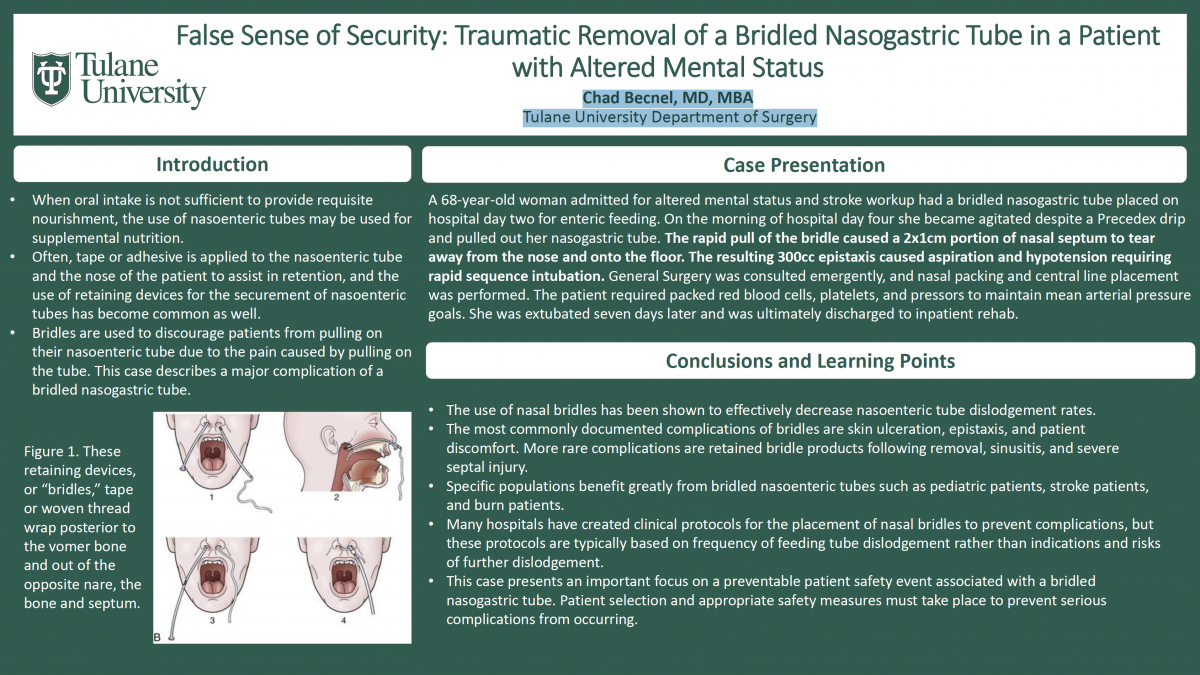
Introduction/Objective: Enteral nutrition plays an important role in the recovery of patients in both acute and chronic medical conditions. When oral intake is not sufficient to provide requisite nourishment, the use of nasoenteric tubes may be used for supplemental nutrition. This technique is frequently used in critically ill patients in an inpatient setting. Accidental dislodgment of nasoenteric tubes is a common issue. Often, tape or adhesive is applied to the nasoenteric tube and the nose of the patient to assist in retention, and the use of retaining devices for the securement of nasoenteric tubes has become common as well. These retaining devices, or “bridles,” tape or woven thread to wrap posterior to the vomer bone and out of the opposite nare, the bone and septum. The ends of a feeding tube are securely connected with the tape. This specific method is primarily used to discourage patients from pulling on their nasoenteric tube due to the pain caused by pulling on the tube. This case describes a major complication of a bridled nasogastric tube.
Case Presentation: A 68-year-old woman admitted for altered mental status and stroke workup had a bridled nasogastric tube placed on hospital day two for enteric feeding. On the morning of hospital day four she became agitated despite a Precedex drip and pulled out her nasogastric tube. The rapid pull of the bridle caused a 2x1cm portion of nasal septum to tear away from the nose and onto the floor. The resulting 300cc epistaxis caused aspiration and hypotension requiring rapid sequence intubation. General Surgery was consulted emergently, and nasal packing and central line placement was performed. The patient required packed red blood cells, platelets, and pressors to maintain mean arterial pressure goals. She was extubated seven days later and was ultimately discharged to inpatient rehab after a thirty-three day hospital course.
Discussion: The use of nasal bridles has been shown to effectively decrease nasoenteric tube dislodgement rates. However, this intervention is not without the risk of serious complication. The most commonly documented complications of bridles are skin ulceration, epistaxis, and patient discomfort. More rare complications are retained bridle products following removal, sinusitis, and severe septal injury. With any intervention, patient selection is vital as a predictor of success. Specific populations benefit greatly from bridled nasoenteric tubes such as pediatric patients, stroke patients, and burn patients. Many hospitals have created clinical protocols for the placement of nasal bridles to prevent complications, but these protocols are typically based on frequency of feeding tube dislodgement rather than indications and risks of further dislodgement. For example, a patient who has pulled their nasogastric tube three times in one week may then “qualify” for a bridle to prevent subsequent self-removal. These protocols fail to consider causality and risk when determining indication for bridle use. Though the benefits of bridles often outweigh the risks, credence must be given to patient mental status and level of agitation prior to placement of a secured device such as a bridle.
Conclusion: This case presents an important focus on a preventable patient safety event associated with a bridled nasogastric tube. Patient selection and appropriate safety measures must take place to prevent serious complications from occurring.