Clinical Science | Surgical Oncology
A Attia, M Youssef, M Omar, M aboueisha, M Shama, E Kandil
ePoster Presenter: Abdallah Attia MD, Tulane School of Medicine
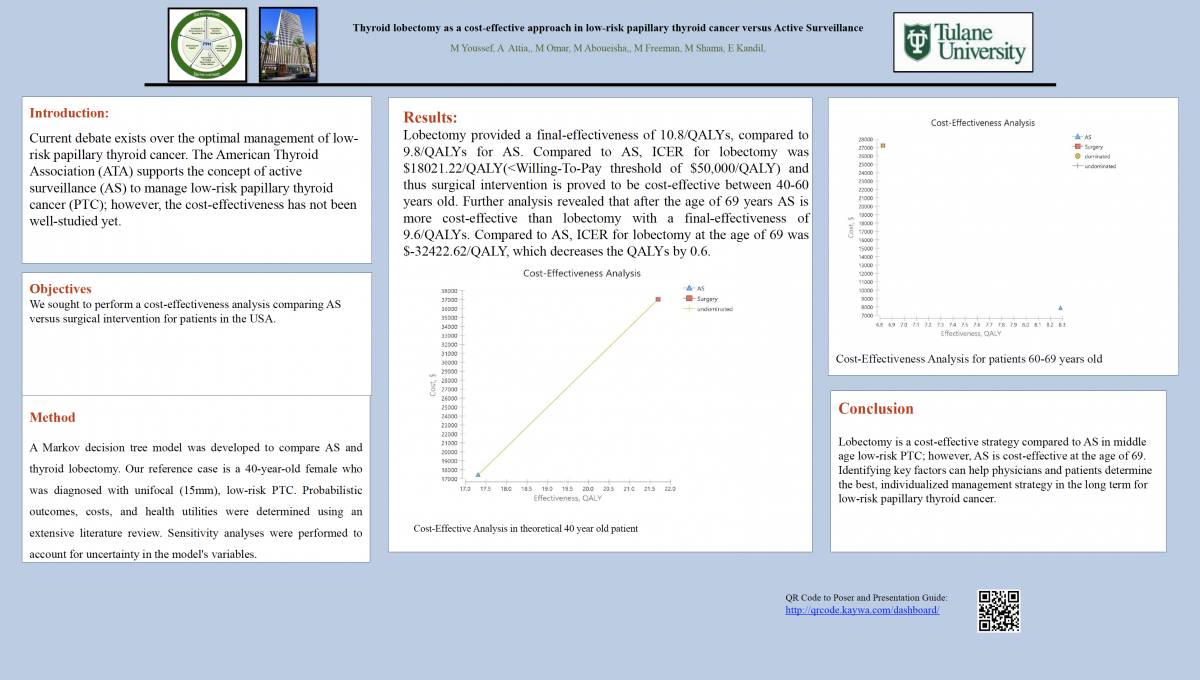
Background: Current debate exists over the optimal management of low-risk papillary thyroid cancer. The American Thyroid Association (ATA) supports the concept of active surveillance (AS) to manage low-risk papillary thyroid cancer (PTC); however, the cost-effectiveness has not been well-studied yet.
Objectives: We sought to perform a cost-effectiveness analysis comparing AS versus surgical intervention for patients in the USA.
Methods: A Markov decision tree model was developed to compare AS and thyroid lobectomy. Our reference case is a 40-year-old female who was diagnosed with unifocal (15mm), low-risk PTC. Probabilistic outcomes, costs, and health utilities were determined using an extensive literature review. Sensitivity analyses were performed to account for uncertainty in the model’s variables.
Results: Lobectomy provided a final-effectiveness of 10.8/QALYs, compared to 9.8/QALYs for AS. Compared to AS, ICER for lobectomy was $18021.22/QALY(<Willing-To-Pay threshold of $50,000/QALY) and thus surgical intervention is proved to be cost-effective between 40-60 years old. Further analysis revealed that after the age of 69 years AS is more cost-effective than lobectomy with a final-effectiveness of 9.6/QALYs. Compared to AS, ICER for lobectomy at the age of 69 was $-32422.62/QALY, which decreases the QALYs by 0.6.
Conclusion: Lobectomy is a cost-effective strategy compared to AS in middle age low-risk PTC; however, AS is cost-effective at the age of 69. Identifying key factors can help physicians and patients determine the best, individualized management strategy in the long term for low-risk papillary thyroid cancer.