Clinical Science | Abdominal/Laparoscopy
F Armstrong, J Savoy, M Curet, R Downey, A Morgan, A Sit
ePoster Presenter: Francesca Armstrong MD, LSU Health – Shreveport
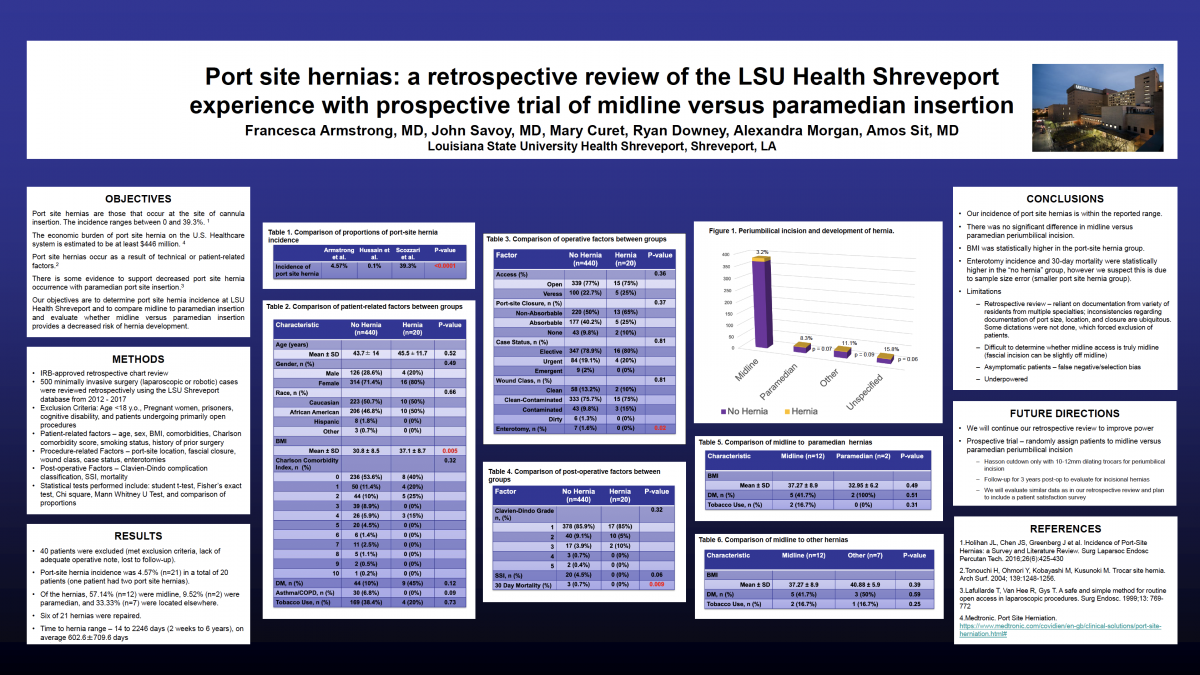
Background: Port site hernias are defined as occurrence of a hernia at the site of cannula insertion. The incidence of port site hernias ranges from 0% to 39.3% according to several series. In recent years, the economic burden of port site hernia on the U.S. healthcare system is estimated to be at least $446 million. It is suspected the occurrence of port site hernias may be secondary to technical factors as well as patient-related factors. Some studies report decreased incidence of port site hernias with paramedian skin incisions as opposed to midline incision.
Objectives: Our objective is to determine port-site hernia incidence at LSU Shreveport, as well as determine whether midline versus paramedian insertion provides a decreased risk of developing port site hernias. We plan to determine our incidence via retrospective review. Eventually, we will carry out a randomized controlled prospective trial to compare midline versus paramedian insertion, and whether one technique has a decreased incidence of hernia compared to the other.
Methods: A total of 520 patients that underwent minimally invasive surgery (laparoscopic or robotic) were reviewed retrospectively. We analyzed patient-related data (i.e. age, sex, BMI, Charlson comorbidity score, smoking status, diagnosis), procedure-related factors (procedure type, port site, port site fascial closure, wound classification, intentional versus unintentional enterotomy), and post-operative factors (Clavien-Dindo Classification, occurrence of surgical site infection, and occurrence of port site hernia).
Results: Out of 520 patients, 53 were excluded secondary to exclusion criteria, lack of adequate operative note, and as well as lost to follow-up. Our incidence of port site hernia was 4.92% (n=23), which is within the range of reported incidence of port site hernias in the literature. Of these, 60.87% (n=14) were midline, 8.7% (n=2) were paramedian, and 30.43% (n=7) were located elsewhere. BMI was significantly higher in the hernia group (37.15±8.72 vs 30.79±8.46, p=0.004). When comparing midline versus paramedian port site hernias, BMI was higher in the midline hernia group, but this was not statistically significant.
Conclusion: Our incidence of port site hernias at LSU HSC Shreveport is within the reported range in the literature. We believe a randomized controlled prospective trial comparing midline versus paramedian umbilical port-site placement could help determine if either has a decreased risk of port-site hernia.