Clinical Science | General Surgery
Stacey Lynch, Jennifer Kim, Seth Fruge, and Forrest D. Griffen.
ePoster Presenter: Stacey Lynch MD, LSU Health – Shreveport
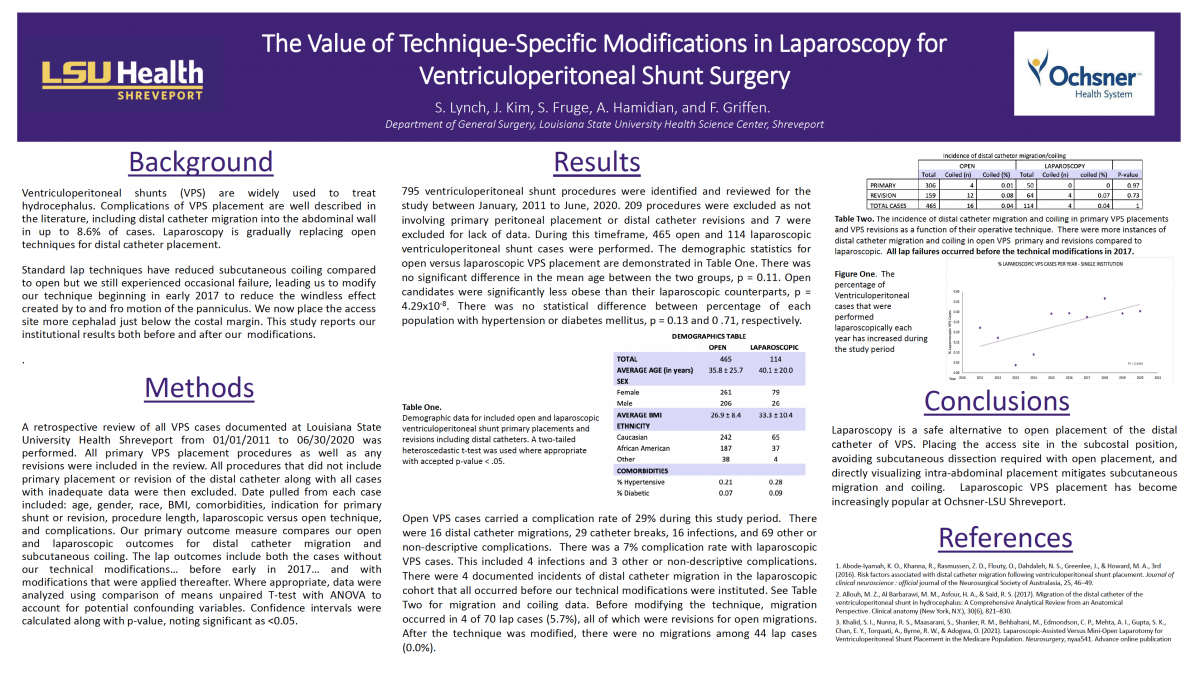
Background: Ventriculoperitoneal (VP) shunts are cerebral shunts that drain excess cerebral spinal fluid (CSF) into the peritoneal cavity when there is an obstruction of normal outflow or decreased CSF absorption. VP shunts are commonly used in treating hydrocephalus in both children and adults. Complications of VP shunt placement are well described in the literature, including distal catheter migration into the abdominal wall. These complications result in decreased VPS efficacy, increased OR trips for VPS revisions, increased healthcare costs, and ultimately – poorer patient outcomes.
Objectives: In this study, a novel technique in laparoscopic distal VPS placement is described and compared with open as well as standard laparoscopic techniques, hoping to show that this method of distal VPS catheter placement can reduce the incidence of distal catheter complications and, in particular, catheter migration and coiling into the abdominal wall.
Methods: After obtaining institutional review board approval, a retrospective review of all VPS cases at Louisiana State University Health from 01/01/2011 to 06/30/2020 was performed. All primary VPS placement procedures as well as any revisions were included in the review. All procedures that did not include primary placement or revision of the distal catheter were then excluded. Data point pulled from each case included: Age, gender, race, BMI, comorbidities, indication for primary shunt or revision, procedure length, laparoscopic versus open technique, complication, and follow-up. The primary outcome studied was the incidence of distal catheter migration and coiling using our modified, technique-specific laparoscopic approach versus open and standard laparoscopic techniques. Where appropriate, data were analyzed using comparison of means unpaired T-tests with ANOVA where appropriate to account for potential confounding variables. Confidence intervals were calculated along with p-value, noting significant as <0.05.
Results: 866 shunt procedures were identified and reviewed for the study. Procedures not involving primary peritoneal placement or distal catheter revisions were excluded. Demographic statistics will be calculated to demonstrate the population characteristics of open versus laparoscopic versus modified laparoscopic techniques. The incidence of complication between open, laparoscopic, and modified laparoscopic techniques will be calculated and statistically compared. Complications of distal peritoneal catheter migration will be calculated and compared between the three techniques. Early review of these data points has suggested better outcomes with laparoscopy for both primary shunt placement and distal catheter revisions.
Conclusion: Laparoscopy is a safe alternative to open placement of the distal catheter of VPS. Placing the access site in the subcostal position and avoiding subcutaneous dissection as required with open placement mitigates migration and coiling.