Clinical Science | Dialysis Access
Y Nakagawa, K Alabaster, A Paramesh
ePoster Presenter: Yusuke Nakagawa BS, Tulane School of Medicine
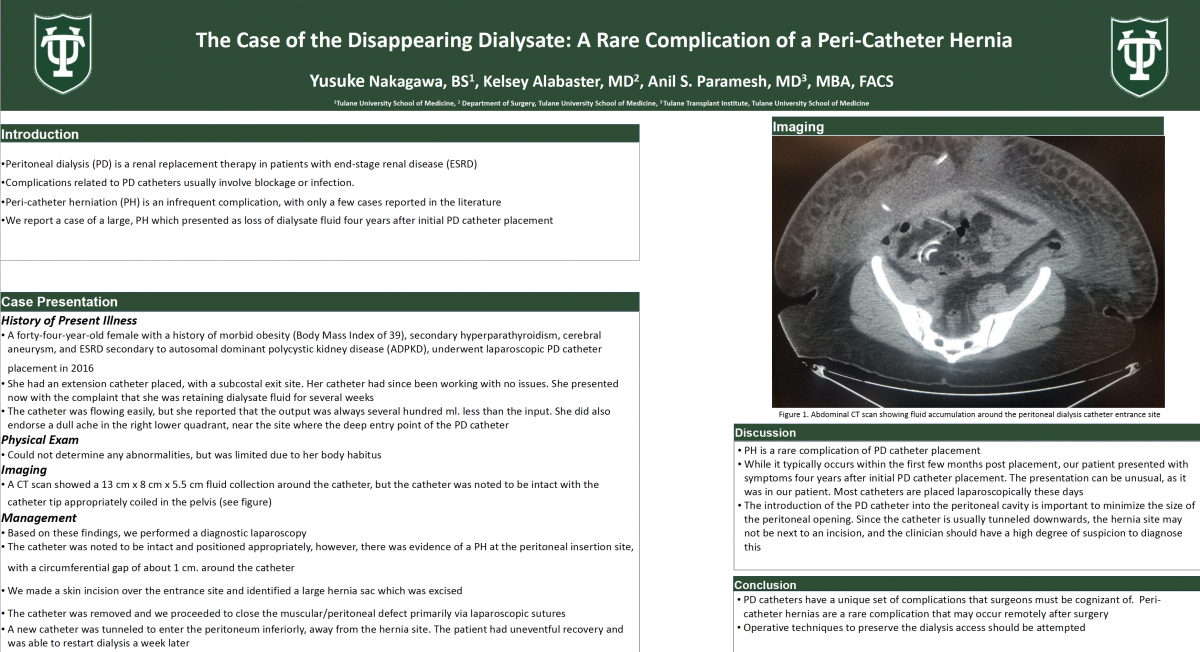
Introduction/Objective: Peritoneal dialysis (PD) is a renal replacement therapy in patients with end-stage renal disease (ESRD). Complications related to PD catheters usually involve blockage or infection. Peri-catheter herniation (PH) is an infrequent complication, with only a few cases reported in the literature. We report a case of a large, PH which presented as loss of dialysate fluid four years after initial PD catheter placement.
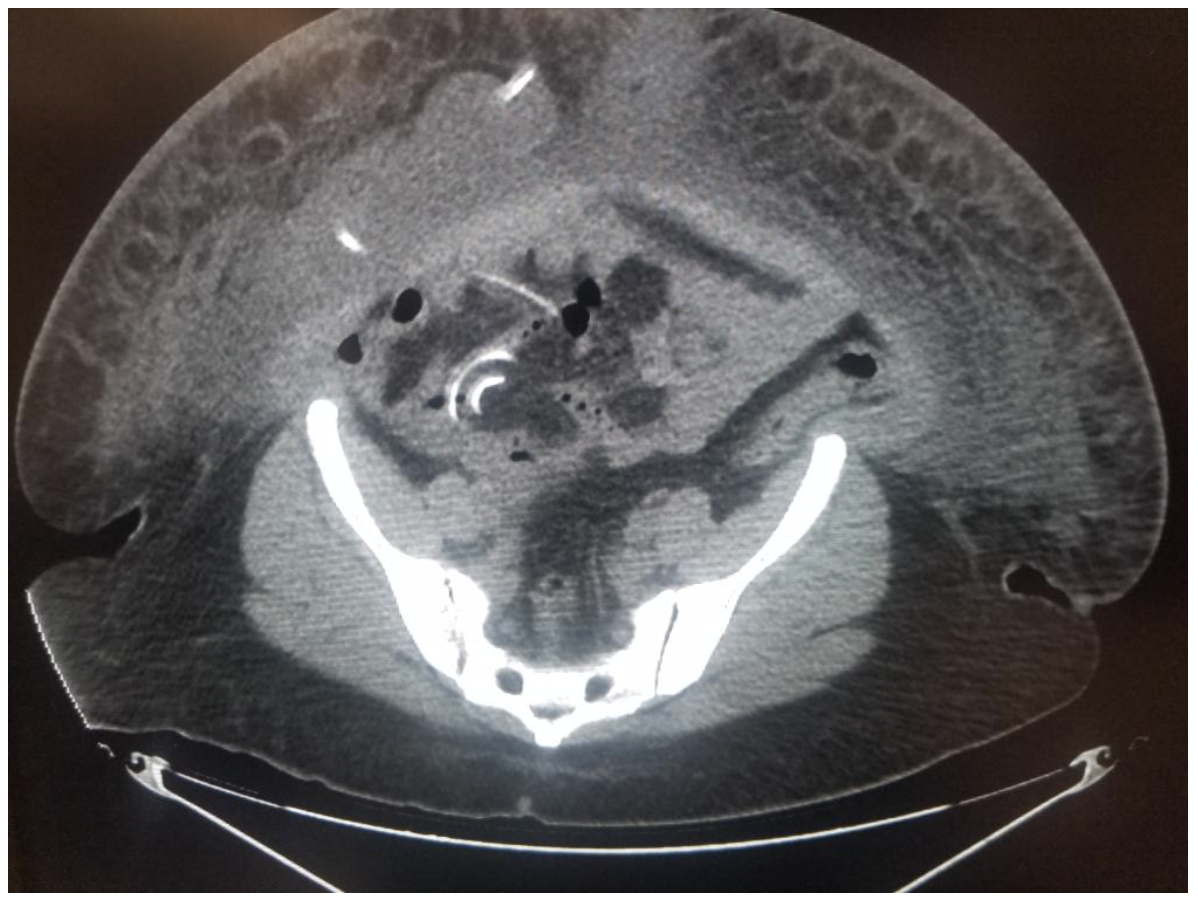
Case Presentation: A forty-four-year-old female with a history of morbid obesity (Body Mass Index of 39), secondary hyperparathyroidism, cerebral aneurysm, and ESRD secondary to autosomal dominant polycystic kidney disease (ADPKD), underwent laparoscopic PD catheter placement in 2016. She had an extension catheter placed, with a subcostal exit site. Her catheter had since been working with no issues. She presented now with the complaint that she was retaining dialysate fluid for several weeks. The catheter was flowing easily, but she reported that the output was always several hundred ml. less than the input. She did also endorse a dull ache in the right lower quadrant, near the site where the deep entry point of the PD catheter. Physical exam could not determine any abnormalities, but was limited due to her body habitus. A CT scan showed a 13 cm x 8 cm x 5.5 cm fluid collection around the catheter, but the catheter was noted to be intact with the catheter tip appropriately coiled in the pelvis (see figure). Based on these findings, we performed a diagnostic laparoscopy. The catheter was noted to be intact and positioned appropriately, however, there was evidence of a PH at the peritoneal insertion site, with a circumferential gap of about a cm. around the catheter. We made a skin incision over the entrance site and identified a large hernia sac which was excised. The catheter was removed. We proceeded to close the muscular/peritoneal defect primarily via laparoscopic sutures. A new catheter was tunneled to enter the peritoneum inferiorly, away from the hernia site. The patient had uneventful recovery and was able to restart dialysis a week later.
Discussion: PH is a rare complication of PD catheter placement. While it typically occurs within the first few months post placement, our patient presented with symptoms four years after initial PD catheter placement. The presentation can be unusual, as it was in our patient. Most catheters are placed laparoscopically these days. The introduction of the PD catheter into the peritoneal cavity is important to minimize the size of the peritoneal opening. Since the catheter is usually tunneled downwards, the hernia site may not be next to an incision, and the clinician should have a high degree of suspicion to diagnose this.
Conclusion: PD catheters have a unique set of complications that surgeons must be cognizant of. Peri-catheter hernias are a rare complication that may occur remotely after surgery. Operative techniques to preserve the dialysis access should be attempted.